Information Technology Issues in electronic healthcare records
Question
Greenway Medical Technologies: The Pace-Setting David of Electronic Health Records
The above case study outlines the potential value offered by electronic healthcare records (EHR) but also raises a number of issues. The case material is comprehensive but, in essence, focuses on the improving the management of doctors’ offices through the application of information technology and systems. The requirement for this case study is to analyse the IT value issues of EHR so that a business case can be developed for management of a doctor’s practice.
You are required to analyse the case material provided to you and produce a report to management with the title: The Business Case for Investing in EHR within a Doctor’s Practice. You should identify the issues in the case material that have relevance to a business case and produce a written report from the information available. To understand the issues associated with EHR you should not only rely on the information provided in the case study but also conduct your own research. EHR is very topical and there is much information available through the ECU e-library. A sample journal article relevant to the topic titled “Information Technology Issues in Healthcare: Hospital CEO and CIO Perspectives” is provided with the case material.
You must also consider the ethical and social implications of the implementation of such as system.
Answer
1. Background information: A general practitioner plays a vital and crucial role in a society, as they are responsible for analysing the health of their patients. They are destined to provide proper care and medications to their patients by diagnosing their issues. Therefore, they have immense responsibilities within healthcare environment, as they need to understand their patient's pain including the social attributes. There are situations when doctors need to take decisions regarding patient’s health and therefore, their appropriate diagnosis is prerequisite. Aboujaoude & Starcevic (2015) commented that in order to take decision regarding patient’s health, sometimes they require assistance. This requirement for assistance depends on the nature of illness of their patients. Erb et al. (2015) opined that doctors apart from recovering the patient from illness provide ample knowledge and information to these patients so that they could lead a healthy life. Doctors are also allocated with tasks to deal with the patient's family members as they become anxious with their patient's health. Therefore, in all spheres of medical environment, doctors play a major role in recovering their patient's health and provide them with normal pain-free life.
These general practitioners need to record their patient's health status for future usage. There are scenarios where doctors need to refer to other doctor and therefore, these records are essential. These referred doctors need to understand their patient's medical history and therefore, these recordings are vital. Duckett & Willcox (2015) have commented that this collection of records needs to be error-free as it involves data of patients. Incorrect information regarding patient's health could affect the health and diagnostic technique of their patients. Moreover, wrong information about health could also delay the analysis made by doctors. Therefore, in order to make the analysis and recording of patient's information, doctors have used various technologies and tools. These would help the doctors to record the patient's health status effectively. The electronic health record is one of the automatic techniques used by doctors to record their patient’s health effects. Gimbel et al. (2017) opined that electronic health records sometimes use cloud technology in order to secure information that is stored within it.
Furthermore, Allen & Flack (2016) opined that this use of cloud technology help the doctors to secure their patient's information without fearing any third party intervention.
Moreover, this electronic health records also uses several other promising technologies in order to secure and store medical information. Doctors need to record the medical history along with medications and this would help other doctors to provide proper treatment and care to these patients. In Australia, Medlink health record offers several tools and techniques in order to help securing patient information. This software is easy to use by doctors and therefore, this us user-friendly. This automatically generates letters from the consultation letters of doctors (Ben-Assuli, 2015). Therefore, doctors do not generate manually data. Moreover, this software has an additional feature where doctors could hand-draw images within the file and this software stores information regarding pathology, medications along with general notes related to their patients.
2. Executive summary: Healthcare professionals have several issues while documenting their patient’s data. This report has been created in order to align the needs and requirements of the patients. Doctors use manual paper documentation in order to store information regarding patient's data. In recent years, there has been an upsurge of the use of technology. People tend to become more dependent on the use of technology and therefore, this has been implemented in this medical profession. In order to ease doctors, doctors to store patient information have used electronic health records. Medical history of patients needs to be assessed by doctors and it is merely not possible to bring all the manual paper files by these patients. However, this paper documentation tends to be expensive and fragile. EHR uses cloud-based computing technology that secure information from any third party intervention. Therefore, this helps the doctors to secure information regarding patient's health. Since, in this case, less time is required, therefore; doctors count concentrate more on their patients in providing medications.
The use of EHR saves time and therefore, this is prerequisite in case of medical environment. The doctors, as well as staff members, need to be provided with proper training regarding the use of documentation procedure. Several nonfinancial tasks like appointments and invoicing are performed by this EHR. These electronic health records automatically update data and information related to their patients. A major limitation of this review is a limited number of references used. This EHR has immense benefits apart from storing information. Medilink is one of these electronic records that secures information and stores data regarding patients. Henceforth, the use of this EHR is beneficial in case of doctors in securing information.
3. Key recommendations: Doctors or general practitioners need to ensure proper handling of information and data related to their patients. This would further assure patient’s sound health and proper diagnosis of their illness. Therefore, in order to make this task easier, electronic health records have been discovered. These records would provide all the required credentials of their patient’s medications and illness so that doctors do not find any issue while medicating their patients. However, it has been seen that these doctors often face various issues while delivering services to their patients and therefore, some recommendations are provided below that could ease the doctors handling these records.
Primary recommendations: In medical environment, patient's health is prerequisite and therefore, the doctors need to assure proper recording and securing of data related to their patients. Adler et al. (2016) commented that these records are critical, as they would enlighten the doctors regarding their patient's status of health. However, there are situations where these doctors mishandle these recordings and this affects the health of their patients.
- Some of the doctors fail to record their patient’s detail. Claggett, Watson & Boudreau (2011) commented that some of the doctors manually record their patient's data and therefore, errors occur. Henceforth, it is recommended for these doctors to use electronic health recording as these software records data automatically from doctor’s consultation reports.
- Sometimes patient’s data need to be changed and edited for the betterment of the doctors. Therefore, this EHR provides an additional advantage as they could automatically get updated with correct information. Any doctor could change information within these databases and therefore, this would provide an additional database to these doctors.
- Consulting with other doctors could also be done effectively with the help of this EHR. Some of the patient’s health gets critical and therefore, one doctor is not enough to handle the situation. In such scenarios, multiple doctors are consulted and therefore, this EHR is crucial and serves to ease the consulting process. It is recommended to use this EHR as doctors at any point in time can assess it.
Secondary recommendations: Apart from medications and consultation, doctors and staff members need to appoint, invoice and claim various processes. The staff members perform these functions. Apart from securing and storing information and data, electronic health records are also used for appointment purposes.
- It is recommended to use EHR in order to manage appointments. Gajanayake, Iannella & Sahama (2014) commented that it is not possible for any staff members or doctors to remember the total number of patients or schedule their appointments. EHR is essential as it could automatically update information and schedule appointment details of any patient. Therefore, the doctors do not need to worry regarding the appointments, as this would be done automatically by EHR.
- Doctors need to customize details about their patient’s information and format styles. Therefore, this EHR would help these doctors to customizer patient's details as per the requirement of doctors.
- Invoices need to be generated by staff members of every patient and therefore, manual invoice generation could be full of errors. In this case, EHR could help the doctors as well as staff members to generate invoice automatically.
4. Strategic context: One of the main roles of these general practitioners is to provide continuous benefits to their patients so that they do not get affected. It is essential to provide appropriate medications and care to their patients so that their health gets improved. Patient's health is one of the prerequisites of any doctors and their information and data needs to be secured appropriately.
These practitioners need to check these data properly before implementing them. Gellert, Ramirez & Webster (2015) commented that these records would include details about medication and therapies that are administered to patients. Cohen et al. (2013) argued that every patient have medical history and therefore, most of the doctors record inappropriately. Henceforth, doctors need to use electronic health records in order to secure and store information. Kerai, Wood & Martin (2014) commented that this storing information with the help of software is essential as they could be operated automatically. Furthermore, Elmore et al. (2016) argued and commented that these doctors before storing data and medical record need to review this information. This form of reviewing data is essential in order to validate data. Therefore, it is usually recommended to use digital health records, as these generally do not possess any issue.
In case of manual health record collection, patients need to carry health files to their doctors and these doctors need to study the entire files before diagnosing the patients to understand their health issues. Furthermore, in case of multiple files, these patients need to carry many files at a time and therefore, this creates a major problem. The doctors need to study the files and then medicate the patients and sometimes reading files may become risky and complicated. Therefore, Adair et al. (2016) opined that in such scenarios, patient’s data if recorded in some software then the patients do not need to carry files.
Current state- The following are some of the current practices that are prevalent in health care centres and their related issues are discussed-
- Manual and paper documentation is complicated and risky. There are health care centres that prefer to store data and information in the form of paperwork and this requires a lot of space. Moreover, this paperwork is generally expensive and therefore, this overall affects the health care system.
- Doctors often take time in reviewing medical history of patients. Weber et al. (2018) opined that patients generally have huge files of their medical history and therefore, it often takes time for these doctors to review them and accordingly provide medications.
- Reviewing files often reduce the production rate of the doctors. The doctors could not provide proper medications to their patients. Therefore, this overall affects the health status of the patients.
- Paper documentation is fragile and they could be lost. These paper works could get damaged easily and therefore, this affects the health of the patients. Doctors will not be able to prescribe medications to these patients in case medical history gets lost. Therefore, this ultimately affects the health of the patients.
- It is difficult for files to share and therefore, it becomes difficult for other doctors to understand the medical history of the patients. Nguyen, Bellucci & Nguyen (2014) opined that this paper documentation is also difficult to edit or change. Therefore, current documentation is difficult to process.
Therefore, it has been seen from the above-mentioned constraints that the doctors face various issues while dealing with paper documentation. Doctors need to ensure proper documentation of their patient's data so that they could be assessed properly in future without having any issues.
Future state- The future needs of doctors within the healthcare system are as follows-
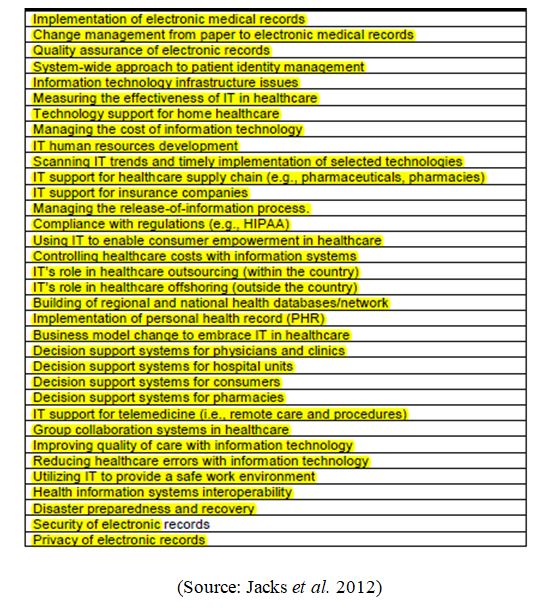
- An environment that is flexible and suitable for the doctors. Jacks et al. (2012) commented that appropriate environment is essential with healthcare facilities that could facilitate better healthcare system.
- The healthcare facilities need to use a virtual system so that doctors could use from remote locations.
- Doctors prefer to use software that could help them to access patient's data quickly. While prescribing medications, doctors need to use medical records and therefore, documentation needs to be quick and faster.
- Doctors need to use such software of recording data that are user-friendly and do not take much time to understand. Gourevitch et al. (2015) opined that medical practitioners do not have adequate time to get knowledge regarding the user of these software therefore, they need to be easy-to-handle.
- Paper-based documentation needs to be replaced by new technologies that could be handled easily. Furthermore, these technologies need to be used by doctors, nurses as well as staff members. Majeed et al. (2015) have commented that these technologies need to be easily accessed by these individuals.
- These technologies need to be easily used and accessed by doctors and the outcome needs to be understood appropriately by every member.
- The technologies need to be assessed by staff members while they are traveling. Patient’s appointment needs to be done by staff members and therefore, these technologies need to be assessed by staff members at any time. [Refer to Appendix 1]
It has been seen that doctors need to use electronic records, as this would mitigate the issues faced by these doctors. Furthermore, Cahill & Makadon (2014) have commented that these practitioners need to secure the data and information related to their patients. Medilink is one of the health record vendors that offer variety of services. Kush et al. (2015) opined that electronic health records serve many benefits as they could secure information of the health care status of the patients.
Mitigation steps- The reasons and the major benefits that these electronic health record serves have been formulated as below-
- This electronic record regularly updates and alters the doctors regarding their patient's health. These records contain details about their patient's health so that they could provide proper medications to their patients based on their health.
- Appointments are made easier with the help of these electronic health records. Dudley et al. (2016) commented that these electronic health records could even prepare invoices of patients. Therefore, staff members do not need to generate manual invoices.
- Electronic records could be easily updated with patient's history. Therefore, updating any patient's data is no difficulty in case of EHR. Sudlow et al. (2016) opined that there is some information that needs to be updated as per the patient's health. This becomes difficult in case of paper documentation. Therefore, these electronic health records serve to benefit the doctors regarding documenting patient's details.
- In case any appointment needs to be cancelled or rescheduled, electronic health records are essential. Therefore, this sort of recording and documentation is beneficial for the doctors.
- Medilink contains details of the pathology as well as medication history of patients. Therefore, this is useful for the patients and doctors to remember the type of medications that are provided to the patients. Aboujaoude & Starcevic (2015) opined that documentation of medications also help the doctors to provide treatments and care based on the current state of the doctors.
Therefore, it is essential for these doctors to secure information and data using electronic health records. Moreover, these records work under cloud technology and therefore, this helped in securing their data. It is the duty of the doctors and staff members to ensure and protect details of their patients. Therefore, this EHR is beneficial for these doctors to secure details of their patients.
5. Analysis of the investment: Electronic health records provide various advantages to its users. This record provides financial benefits as well as quality services to the doctors. EHR provides several financial as well as non-financial benefits to its users. Furthermore, Claggett, Watson & Boudreau (2011) commented that electronic health records do not have any issue regarding their set-up. Medilink is one of the most used Australian software that has various implications for in the healthcare professionals. Moreover, they are quite cost-effective as well as user-friendly. Therefore, the professionals do not have any issue with their setup. Moreover, being user-friendly, this software could be used by staff members.
Financial benefits: It has been seen that in case of Medilink, the starting price is about AUD 950 and this is the first time payment. Furthermore, Gajanayake, Iannella & Sahama (2014) commented that once installed, this software would not have any further issue with their implementation. Doctors find these easy to handle and therefore staff members could easily use this software. Free version of this software is easily available and therefore, installing this software is not an issue. Doctors could easily install this software and use them without paying. Therefore, with the help of this free version, doctors could easily use this without any payment. Moreover, this software is based on cloud Saas and therefore storing data is beneficial and easier.
Non-financial benefits- Medilink provides various advantages to its users. This documentation records all essential data and information of the patients. Gellert, Ramirez & Webster (2015) opined that this record stores information regarding patient's health and alert doctors regarding their illness. These health records generate consultation letters automatically. Cohen et al. (2013) commented that these electronic health records review the history of the patients. Therefore, this allows the doctors to understand their patient's illness merely by looking at the documentation. Understanding and detailed information related to patient's radiology and general letters are essential and this medilink stores information, thereby allowing doctors to mediate properly. As a result, these documentations are essential for securing and storing patient data that could be used by other doctors. Sometimes patient’s health becomes serious and in those circumstances, securing information is essential that could be revised by the doctors.
Implementation risks: In order to set up this medilink software, there are certain risk factors that need to be determined while installing this software. The following are some of the risks factors that occur at the time of implementation of this software.
- Setting up EHR software does not require any pre-installed equipment. However, it has been seen that the current equipment may not get compatible with the installed software.
- Sometimes during verifying this software, billing issues occur and this causes mismatch of information related to patient’s data.
- Doctors, as well as staff members, need to be properly trained on using this software so that no confusion exists at the time of documentation of patient's data.
- Regular update of the software is vital and essential for this technology to work better.
- Encryption of data is vital as the information stored in this recording software could be intervened by third party. Therefore, proper installing cloud computing system or encrypting of data are essential in order to store and secure data and information.
However, besides these above-mentioned risk factors, another major risk of this implementation is resistance by the doctors and staff members. Staffs might be unwilling to implement this software as these might affect and change their habits. It is essential to train the doctors as well as staff members before implementing this software.
6. Benefits of realization: The hospital staff members and doctors are the end users of this EHR. Therefore, one of the major benefits of this implementation is a change in the entire management within the healthcare unit. These members need to have adequate training regarding this implementation of techniques and software before using them. This would imply proper usage of this software. Kerai, Wood & Martin (2014) opined that this EHR could also be used in order to supervise project life cycle. Therefore, this implementation of EHR has immense benefits in terms of securing information of patients that ultimately improves the health status of them.
7. Ethical and social implications: The doctors need to ensure proper documentation of information related to their patients. Elmore et al. (2016) have commented that doctors need to seek permission from patient’s family members before consulting with other doctors. Therefore, information or data regarding patient's medical history should not be disclosed to other doctors as per the Data Protection Act 1998. One of the potential risks related to the use of this EHR is intervention by their party. Proper encryption of data and use of cloud computing technology are essential in order to store information and data (Journals of Health & Medical Informatics, 2018). Therefore, the doctors need to be properly trained regarding the use of this EHR.
8. Limitations: The major limitation of this review is inadequacy of data and information regarding the use of this EHR. Moreover, the databases included in this study had login constraints that restricted the usage of data and information (Cahill & Makadon, 2014). There were lower numbers of references that have been used in this article band this also served as other major limitations of this study. Henceforth, a proper analysis of the use of EHR and their benefits could not be analysed appropriately.
Reference List
Books
Aboujaoude, E., & Starcevic, V. (Eds.). (2015). Mental health in the digital age: grave dangers, great promise. Oxford University Press. Retrieved from http://bit.ly/2LtWYRu
Blais, K., Hayes, J. S., Kozier, B., & Erb, G. L. (2015). Professional nursing practice: Concepts and perspectives (p. 530). NJ: Prentice Hall. Retrieved from https://smrth1tyx01.storage.googleapis.com/MDEzMzgwMTMxNA==01.pdf
Duckett, S., & Willcox, S. (2015). The Australian health care system (No. Ed. 5). Oxford University Press. Retrieved from https://www.cabdirect.org/cabdirect/abstract/20173279780
Lowry, S. Z., Lowry, S. Z., Ramaiah, M., Prettyman, S. S., Simmons, D., Brick, D., ... & Gimbel, K. (2017). Examining the Copy and Paste Function in the Use of Electronic Health Records. US Department of Commerce, National Institute of Standards and Technology. Retrieved from https://nvlpubs.nist.gov/nistpubs/ir/2017/NIST.IR.8166.pdf
Journals
Allen, J., & Flack, F. (2016). Evaluation in health promotion: thoughts from inside a human research ethics committee. Health Promotion Journal of Australia, 26(3), 182-185. Retrieved from http://bit.ly/2J0JFtF
Ben-Assuli, O. (2015). Electronic health records, adoption, quality of care, legal and privacy issues and their implementation in emergency departments. Health Policy, 119(3), 287-297. Retrieved from https://www.healthpolicyjrnl.com/article/S0168-8510(14)00329-7/abstract
Casey, J. A., Schwartz, B. S., Stewart, W. F., & Adler, N. E. (2016). Using electronic health records for population health research: a review of methods and applications. Annual review of public health, 37, 61-81. Retrieved from https://www.annualreviews.org/doi/full/10.1146/annurev-publhealth-032315-021353
Claggett, J. L., Watson, R. T., & Boudreau, M. C. (2011). Greenway Medical Technologies: The Pace-Setting David of Electronic Health Records. CAIS, 29, 17. Retrieved from https://pdfs.semanticscholar.org/55b1/ba094b7b879d02d7f2b92e2286ed26a5c304.pdf
Gajanayake, R., Iannella, R., & Sahama, T. (2014). Privacy oriented access control for electronic health records. Electronic Journal of Health Informatics, 8(2), 15. Retrieved from https://eprints.qut.edu.au/48992/1/DUMW2012_-_Paper_2.pdf
Gellert, G. A., Ramirez, R., & Webster, S. L. (2015). The rise of the medical scribe industry: implications for the advancement of electronic health records. Jama, 313(13), 1315-1316. Retrieved from http://medstaff.aahs.org/wp-content/uploads/ScribesJAMAintern2015.pdf
Howard, J., Clark, E. C., Friedman, A., Crosson, J. C., Pellerano, M., Crabtree, B. F., ... & Cohen, D. J. (2013). Electronic health record impact on work burden in small, unaffiliated, community-based primary care practices. Journal of general internal medicine, 28(1), 107-113. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3539023/pdf/11606_2012_Article_2192.pdf
Kerai, P., Wood, P., & Martin, M. (2014). A pilot study on the views of elderly regional Australians of personally controlled electronic health records. International journal of medical informatics, 83(3), 201-209. Retrieved from http://bit.ly/2IMqfoG
Lee, B. S., Walker, J., Delbanco, T., & Elmore, J. G. (2016). Transparent electronic health records and lagging laws. Annals of internal medicine, 165(3), 219-220. Retrieved from http://annals.org/aim/article-abstract/2524809/transparent-electronic-health-records-lagging-laws
MacIntyre, C. R., Menzies, R., Kpozehouen, E., Chapman, M., Travaglia, J., Woodward, M., ... & Adair, T. (2016). Equity in disease prevention: Vaccines for the older adults–a national workshop, Australia 2014. Vaccine, 34(46), 5463-5469. Retrieved from http://bit.ly/2IL9Sgq
McBride, S., Tietze, M., Robichaux, C., Stokes, L., & Weber, E. (2018). Identifying and Addressing Ethical Issues with Use of Electronic Health Records. Online Journal of Issues in Nursing, 23(1). Retrieved from http://bit.ly/2s66l1O
Nguyen, L., Bellucci, E., & Nguyen, L. T. (2014). Electronic health records implementation: an evaluation of information system impact and contingency factors. International journal of medical informatics, 83(11), 779-796. Retrieved from https://www.sciencedirect.com/science/article/pii/S1386505614001233
Palvia, P., Lowe, K., Nemati, H., & Jacks, T. (2012). Information technology issues in healthcare: hospital CEO and CIO perspectives. Information Technology, 5, 1-2012. Retrieved from http://libres.uncg.edu/ir/uncg/f/K_Lowe_Information_2012.pdf
Paul, M. M., Greene, C. M., Newton-Dame, R., Thorpe, L. E., Perlman, S. E., McVeigh, K. H., & Gourevitch, M. N. (2015). The state of population health surveillance using electronic health records: a narrative review. Population health management, 18(3), 209-216. Retrieved from https://www.liebertpub.com/doi/abs/10.1089/pop.2014.0093
Riordan, F., Papoutsi, C., Reed, J. E., Marston, C., Bell, D., & Majeed, A. (2015). Patient and public attitudes towards informed consent models and levels of awareness of Electronic Health Records in the UK. International journal of medical informatics, 84(4), 237-247. Retrieved from http://bit.ly/2IQxTOT
Online Articles
Cahill, S., & Makadon, H. (2014). Sexual orientation and gender identity data collection in clinical settings and in electronic health records: A key to ending LGBT health disparities. LGBT health, 1(1), 34-41. Retrieved from https://pdfs.semanticscholar.org/8dc3/5218acf021b61c48ff99ecc7fa58df1b3adc.pdf
De Moor, G., Sundgren, M., Kalra, D., Schmidt, A., Dugas, M., Claerhout, B., ... & Kush, R. (2015). Using electronic health records for clinical research: the case of the EHR4CR project. Journal of biomedical informatics, 53, 162-173. Retrieved from http://bit.ly/2J8zP94
Miotto, R., Li, L., Kidd, B. A., & Dudley, J. T. (2016). Deep patient: an unsupervised representation to predict the future of patients from the electronic health records. Scientific reports, 6, 26094. Retrieved from https://www.nature.com/articles/srep26094
Zhou, S. M., Fernandez-Gutierrez, F., Kennedy, J., Cooksey, R., Atkinson, M., Denaxas, S., ... & Sudlow, C. (2016). Defining disease phenotypes in primary care electronic health records by a machine learning approach: a case study in identifying rheumatoid arthritis. PloS one, 11(5), e0154515. Retrieved from http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0154515
Websites
Center for Health Journalism (2018). Covering Electronic Health Records. Retrieved from https://www.centerforhealthjournalism.org/resources/lessons/covering-electronic-health-records on 15th January 2018
Journals of Health & Medical Informatics (2018). Electronic Health Record Management: Expectations, Issues, and Challenges. Retrieved from https://www.omicsonline.org/open-access/electronic-health-record-management-expectations-issues-and-challenges-2157-7420-1000265.php?aid=90749&view=mobile on 19th January 2018
Appendices
Appendix 1: Issues of health care facility